Tight glycaemic control reduces the risk of and slows the progression of microvascular and macrovascular complications. A stepped approach is recommended to lower and maintain HbA1c to as close to physiological levels as possible, preferably less than 7%, without hypoglycaemia.
The above comes from
here. The New Zealand guidelines website. This website is a great source of information. I use it heaps. It has enabled me to get and keep reasonably up to speed. Many of those involved in developing these guidelines see them for what they - works in progress - not the final solution. However for many they are - the gospel. They are sourced in an evidence based way and so they must be as close to the truth as we can be for moment. There are some who say
EBM - evidence based medicine - though based on sound principles, has become a religion in some people's hand, potentially dangerous to doctors and patients.
Take the information in the guideline above and compare it to the next two paragraphs which come from what seems like an impeccable source to me.
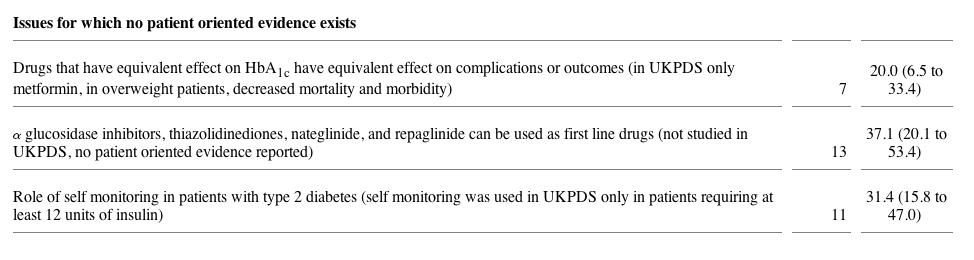
Tight glucose control did not prevent premature mortality or significantly reduce any clinically important diabetes-related complications.
In overweight patients treated with either insulin or sulfonylureas, there was no effect on diabetes-related complications, regardless of the degree of glucose control. (Click here to get full article)
Now I am not an academic or an expert on diabetes. I don't know how to sift B.S. from the good stuff. But the point is very few of us can. And we have all been burnt by what was the truth and now isn't. We have also been burnt by the opinion of experts.
In a recent analysis of review articles on the treatment of type 2 diabetes, we found that the experts writing them often did not tell us—the readers—the most important research evidence published in the past 25 years in the treatment of patients with type 2 diabetes.2 It's time to explore the value of experts and examine our reliance—or even addiction—to the pronouncements of experts.
Don't get me wrong I use the opinion of experts everyday. I couldn't function without them. And I check up on them too!!
In NZ the health managers and others living in airy fairy abstraction land may wonder why doctors aren't doing what's best for their patients, ie follo
wing their rules, ie guide
lines to the letter. Well numero u
no we a
ren't being paid as well as they are in the UK to be obedient robots. There they get paid 12 thousand pounds or so to audit their post heart attack patients for mild depression and then offer them counselling services that don't even exist. Don't believe me read NHS Blog Doc. He has some hilarious stories to tell. Click on him.

There are problems with guidelines. They are not necessarily best practice. They get it wrong sometimes. Even if they are on the mark they change. The truth is not static. Also there can be different interpretations of the evidence - see above. If a doctor is forced to prescribe against what he or she knows to be true, this is not good for their health or their future happiness. The sacrifice of integrity is a high price to pay.
Health managers have taken over the medical profession - well nearly. Guidelines are on the way to becoming rules. We can feeeeeel
it coming. Payment and punishment based on guidelines. Obedience and a loss of integrity can have soul destroying outcomes. No wonder many doctors are not advising their kids to follow them into what is fast becoming a job - rather than a profession.
Doctors really do not want to be force fed and neither do many of their patients. Why should patients obey these guidelines? Really why should they. What is actually in it for them? 99 folk swallow a pill everyday for a year and get zip out of it. Doctors see and patients experience the side effects. Neither experience the benefits.
How long do you have to take BP pills
for before you experience a benefit? You never do experience a benefit. Even if you are one of the lucky ones who would have had a stroke but don't have one, you can not know you would have had a stroke if you hadn't take the pill and so you have no experience of benefit. The doctors don't experience the benefit directly either. Yes your BP may b
e lower but so what - you maybe one of the unlucky ones that gets a stroke anyway. The benefits are theoretical as far as the individual and his doctor are concerned but the side effects are not.
His blood pressure maybe perfect but he has a cough, feels tired and has swollen legs - all caused by the the three different pills he is on. Having a normal blood pressure doesn't make him feel any better. So why should he persist? He knows doctors can be wrong. He knows folk are making money out of him. He's suspicious. He's seen his mate on ten different pills not doing very well. He wants no more pills thanks all the same doctor. Patient non compliance is a major factor. It's not just the doctors fault. And yes many doctors are non complaint too - especially when it comes their turn to take pills - many of them don't even check their own blood presssur
e.
There's another problem with guidelines - how things work in trials with motivated and relatively healthy patients and ambitious researchers/doctors is very different to the real world. Many trials are done on younger and fitter groups than coal face doctors deal with. An 80 year old diabetic with hypertension may have arthritis heart failure reflux and a whole pile of other complaints. By the time each condition is treated they are on a sack load of pills. Polyphar
macy is not a good idea! It's bloody nuts unless a particular patient is highly motivated and well supported it just isn't going to happen. And anyway are the findings in that study relevant to this particular person?
The
HDC , my personal bete noi
r, a government opinion generating organisation, that sits outside normal due process, passed judgement on me on a couple of issues. It took them three years. One of these issues was a dose of valium I
prescribed. This ...... (words don't fail me.It's just what I want to say could land me in hot water) anyway this ........ decided I had used more than a therapeutic dose. How did she know this? She looked in New Ethicals. She blindly accepted what was in that book. She was wrong. Was there anyway of correcting her? Of course not. This opinion, garbage, still sits on my records.
In a few years time guidelines will be used this way too - they probably are already.
Bottom line any system that imposes from top down will in the end fail!! When the boys and girls at the coal face no longer love their work those at the top won't last very long - a couple of generations maybe. They will go out of fashion just like their dreams, visions, ideals, missions and so on. If they want monkeys that's what they will get.

Okay time to stop. I'll get back to the HDC agai
n one day.

 Scarcely two weeks after the Senate overwhelmingly passed legislation touted as a major fix of FDA’s failing effort to assure drug safety, The New England Journal of Medicine published an analysis linking the diabetes drug Avandia to a 40% increase in the risk of heart attack. This finding is especially troubling because people with diabetes are already at high risk of cardiovascular problems. A million diabetics are estimated to be current Avandia users in the U.S.
Scarcely two weeks after the Senate overwhelmingly passed legislation touted as a major fix of FDA’s failing effort to assure drug safety, The New England Journal of Medicine published an analysis linking the diabetes drug Avandia to a 40% increase in the risk of heart attack. This finding is especially troubling because people with diabetes are already at high risk of cardiovascular problems. A million diabetics are estimated to be current Avandia users in the U.S.